

Know the Science: Finding and Evaluating Online Resources
![]()
![]()
![]()
![]()
Meet HRSA's Administrator Thomas J. Engels
Administrator
Health Resources and Services Administration
U.S. Department of Health and Human Services
Thomas Engels is the Administrator of the Health Resources and Services Administration (HRSA). HRSA is the primary federal agency within the U.S. Department of Health and Human Services responsible for improving access to health care for people who are geographically isolated and economically or medically vulnerable.
As the Administrator, Mr. Engels oversees HRSA’s efforts to expand access to quality health care through grants awarded to state and local governments, providers of health profession training programs.
Under Mr. Engels' leadership, HRSA serves more than 31 million people through 1,400 health centers - an essential component of America’s health care safety net– with 15,000 sites in underserved and rural communities that provide primary care services regardless of patients’ ability to pay. Health centers are providing substance use disorder services–behavioral health–in steadily increasing numbers.
Toward that end, the agency continues to grow the behavioral health workforce and recruit providers to underserved and rural communities by investing in growing the National Health Service Corps, which provides loan repayment and scholarships to providers in return for practicing in these high-need communities.
In keeping with its mission, HRSA programs reach more than 60 million pregnant women, infants, and children; more than 560,000 people with HIV; more than 1,900 rural counties and municipalities; and more than 21,000 clinicians in the National Health Service Corps and Nurse Corps and other programs who provide medical, dental and mental health services to over 22 million Americans.
Mr. Engels is the first person to be twice appointed HRSA Administrator by a U.S. President serving nonconsecutive terms.
Mr. Engels was HRSA Administrator from November 2019 until January 2021.
During his initial tenure as administrator, Mr. Engels oversaw programs to address the opioid epidemic through the integration of behavioral health into primary care and HIV care settings. He also directed the management of the historic $175 billion COVID-19 Provider Relief Fund, which provided relief and assistance to hospitals and other health care professionals on the front lines of the coronavirus pandemic. Additionally, he completed the most significant reorganization of the agency in its 40-year history. Mr. Engels also served on the White House Coronavirus Task Force.
Prior to first joining HRSA, Mr. Engels was Deputy Secretary of the Wisconsin Department of Health Services from 2015 to 2019, managing a department with more than 6,000 employees and a $12 billion budget. In that role, he championed and oversaw the expansion of the state’s mental health services, the establishment of a statewide electronic health record system and an increase in staffing at long-term care facilities. He was also an active member of the Governor’s Task Force on Opioid Abuse.
Formerly Vice President of Public Affairs at the Pharmacy Society of Wisconsin, Mr. Engels also served as the Government Affairs Director for the Wisconsin State Telecommunications Association, and previously held public service positions working as Governor Tommy Thompson’s Deputy Press Secretary and Communications Director for the Senate Republican Caucus.
More recently, he was elected as Sergeant-At-Arms by the Wisconsin State Senate in 2021 and re-elected in 2023 and 2025. The Wisconsin State Sergeant-At-Arms is a nonpartisan constitutional officer.
He also is a certified emergency medical technician, and for many years a volunteer firefighter.
Mr. Engels is a native of Wisconsin and holds a Bachelor of Arts degree from the University of Wisconsin-Madison.


Check Out RGSI's Online Portal
The Division of Research, Grants & Scholarly Innovations (RGSI) consists of an administrative core and 3 departments: Sponsored Programs (SP), Research Support (RS), and A.T. Still Research Institute (ATSRI). RGSI is dedicated to nurturing a strong and supportive environment for research and scholarly activity at ATSU.
Sponsored Programs Coaching Memo - ATSU Travel Expense Overview
Sponsored Programs and the Finance Office are delivering a series of grants management coaching memos to support project directors, principal investigators, project teams, ATSU operations teams, faculty, and staff in fiscal management of grants awarded to ATSU.
Topic: ATSU Travel Expense Overview
Summary: This document is intended as an overview of commonly reimbursed expense items from ATSU Policy 50-101: TRAVEL; it is not a substitute for reading and understanding the entire detailed travel policy, which remains the traveler’s responsibility.
Travel expenses that are generally reimbursable (not all inclusive) are listed below.
• Airfare & Taxi: Airline fare for coach/economy rate and applicable taxi fare to and from airport for in- city destinations will be reimbursed. Please provide detailed receipts showing service destination, date, time, and full amount for reimbursement. Always choose the most economical means.
• Meals: Itemized receipts are needed to reimburse meals. Guidance for use of federal grant funds requires a test for reasonable costs of meals. The current limit for federal employees is $68 total per day in the Continental United States (CONUS), therefore ATSU asks travelers to keep meals reimbursed with federal funds around $70 per day. A recommended breakdown of daily meal costs (pre-tax and pre-tip) is included. Alcoholic beverages are prohibited. Tips are allowed up to 20%.
Breakfast: $10.00
Lunch: $20.00
Dinner: $40.00
• Mileage (personal vehicle): Mileage to and from an airport will be reimbursed according to the current IRS-authorized mileage rate. Receipts for gasoline purchases are not needed.
• Rental Car: Midsize rental car fees and gasoline purchases are allowed. No insurance is needed. Always choose the most economical means.
• Lodging: Standard, single occupancy rooms should be secured unless shared with other business travelers. Personal guests must be approved through supervisors or designees and names listed on the invoice.
PLEASE NOTE:
• All travel expenses require an itemized receipt for reimbursement.
• Travelers may upgrade the level of service (airfare, hotel, etc.) at personal expense. ATSU can only reimburse for the economy rate. If upgrading, a screenshot of the economy price before upgrade must be provided; this is the reimbursable amount.
• Tips over 20% must include an explanation for approval consideration.
• Tip amount should be on the subtotal and not on the full taxed amount.
• If necessary to use room service, please request an itemized receipt when ordering. Shared meal receipts must be copied for each person and claimant’s items noted/highlighted on the receipt. Personal guest meals should be removed.
• Employees may pay for meals on behalf of business guests only when there is a business-related purpose. The purpose must be identified and documented at the time of the expense. Additionally, the names of the business guests, along with their relationship (e.g., client, partner, team member), should be clearly identified. This ensures the meal is tied to business activities and can be properly justified.
• Meals without a clear business purpose, or where the purpose and participants cannot be identified,
will not be reimbursed using grant funds.
Summary Conclusion
Grant-related travel expenditures must be administered via the ATSU Travel Policy 50-101 and adhere to the funding source and ATSU travel guidelines and limitations, honoring whichever is most restrictive. All grant related travel must be allowable (as approved in the grant budget), reasonable (no extravagant cost), allocable (easily assigned to the grant objectives), and necessary to complete the project.
ATSU Departments Who Can Help
Sponsored Programs and the ATSU Finance Office can assist with questions regarding grant-funded travel.
Find NIH Funding Information More Quickly and Easily with RCDC's New Look and Feel
NIH recently launched several enhancements to allow the public to more easily and quickly find funding information for various NIH research areas. The new look and feel of the NIH Research, Condition, and Disease Categorization (RCDC) Categorical Spending webpage adds to NIH’s long-standing efforts to enhance transparency and accountability into NIH funding decisions and the research areas NIH supports.
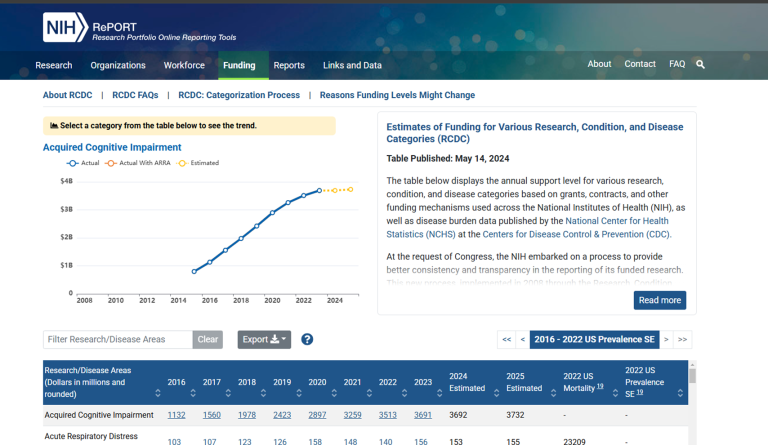
RCDC launched in 2008 as a tool within NIH’s Research Portfolio Online Reporting Tools (RePORT) suite. It provides estimates of annual support level for more than 300 research, condition, and disease categories based on grants, contracts, and other funding mechanisms used across the NIH, as well as disease burden data published by the CDC National Center for Health Statistics.
The new visual and contextual changes aim to improved usability and understanding of the RCDC categorization process. In particular, the categorical spending page was reorganized so data are more prominent and easier to navigate.
Navigation improvements simplify finding information on FAQs, the Categorization Process, and the biomedical thesaurus. The information in the data tables are more visible due to collapsed textual information and frozen table headers (Figure 1).
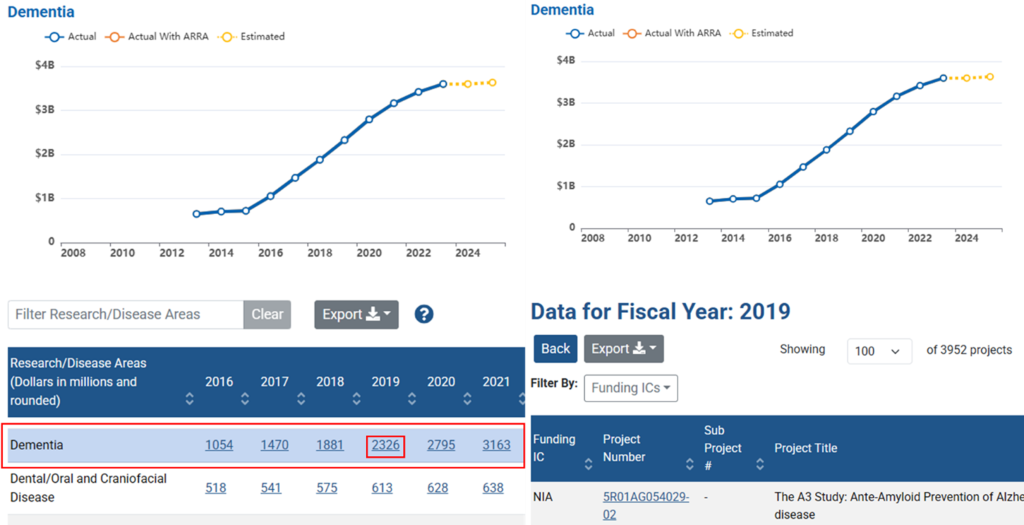
When selecting a particular category, the line graph on the top left of the page will automatically adjust to reflect funding amounts over time for that topic area (Figure 2, left image). Selecting support data for a given fiscal year will also reveal information about specific projects (Figure 2, right image).
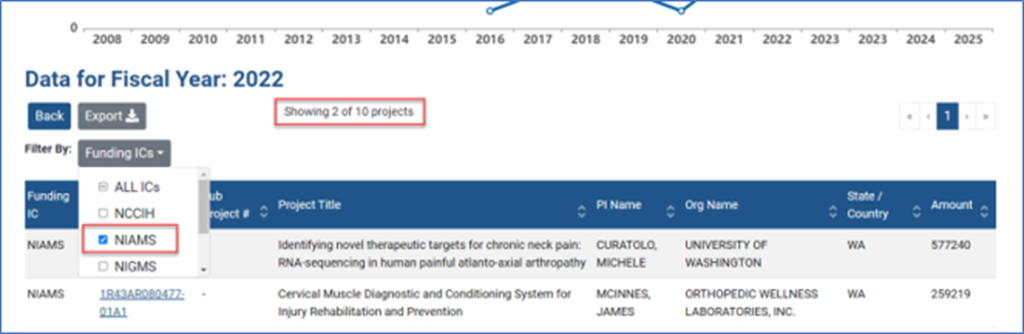
Results can be narrowed further if interested in a particular NIH Institute or Center (Figure 3). To sort in this way, a user would need to click on the dollar amount for a given disease/research area and a given fiscal year in the main table.
Application identification numbers can now be exported for funded awards for any fiscal year in any given category. Previously, RCDC only reported the project number for an award. Because application IDs are unique to an individual fiscal year, it is easier to now connect results from RCDC with those obtained in other RePORT tools.
Questions? report@od.nih.gov
Categories: New Resources
Topics: RePORT/RePORTER
The Whole Person Health Index: A New Tool for Human Mechanistic and Clinical Studies
The Whole Person Health Index is a new tool for human mechanistic and clinical studies.
In human mechanistic and clinical research, the importance of valid, reliable measurement tools to track an individual’s health trajectory over time—assessing improvement or decline—cannot be overstated. Many current clinical measurements focus narrowly on specific organ functions (like blood pressure) or symptoms (like pain), reflecting an approach to health care traditionally organized around distinct diseases affecting different body systems. A major hurdle to research on integrative health has been measurement: How can we reliably assess and consistently track the health of the whole person over time?
The National Center for Complementary and Integrative Health (NCCIH) champions a whole person approach characterized by support for a healthy lifestyle and promotion of positive health processes spanning across multiple body systems.
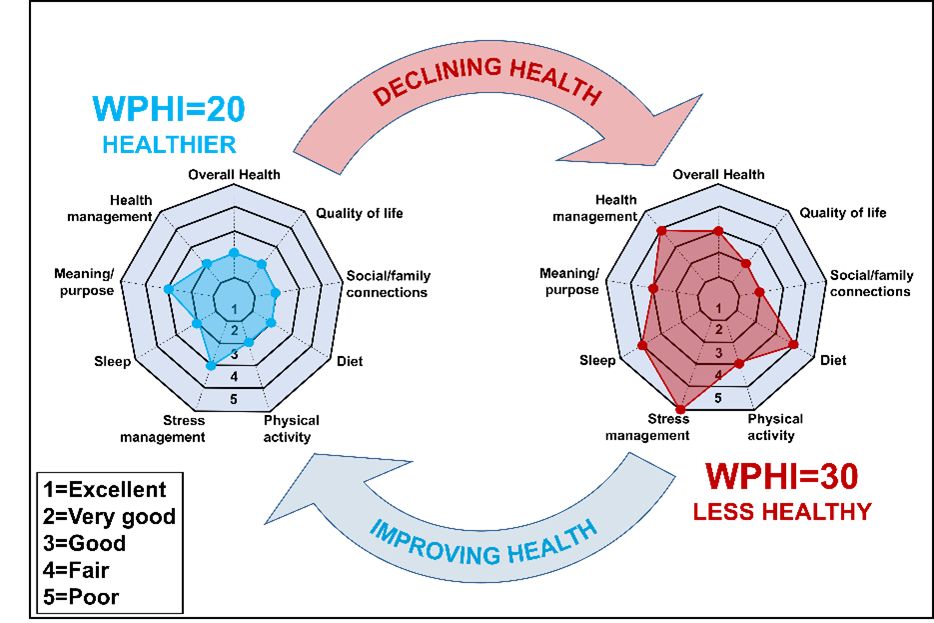
NCCIH and the National Center for Health Statistics at the Centers for Disease Control and Prevention (NCHS/CDC) have developed the Whole Person Health Index (WPHI). The WPHI comprises the following set of nine validated, self-reported questions covering major domains of health.
Whole Person Health Index (WPHI)
Rate on a scale of 1–5 (1=Excellent, 2=Very Good, 3=Good, 4=Fair, 5=Poor)
1. Would you say your health in general is excellent, very good, good, fair, or poor?
2. How would you rate your quality of life, focusing on what matters most to you?
3. How would you rate your social and family connections?
4. In general, how healthy is your overall diet?
5. How would you rate your physical activity, compared with people in your age group?
6. How would you rate your ability to manage stress?
7. How would you rate your sleep?
8. How would you rate your ability to find meaning and purpose in your daily life?
9. How would you rate your ability to manage your health, focusing on aspects of your health that matter most to you?
The WPHI is free to use and is set to be deployed in the 2025 National Health Interview Survey, as well as the All of Us longitudinal cohort. The WPHI can be calculated by summing the nine response scores. For example, an increase of WPHI from 20 to 30 would indicate worsening health, and a reduction from 30 to 20 would indicate improvement in overall self-assessed health.
NIH encourages investigators to use the WPHI as a secondary outcome in research involving human participants, be it a longitudinal observational study or a randomized clinical trial. The WPHI may be particularly valuable in studies evaluating the effects of nonpharmacologic nutritional, psychological, and physical interventions, especially when used in combination. While such interventions often have small-to-medium effect sizes when assessed using a single primary outcome (e.g., pain), they may also exhibit many modest effects across multiple secondary outcomes (e.g., sleep, physical function, quality of life). Using the WPHI as an integrated measure may reveal important additive benefits of these interventions on the health of the whole person.
Implementation of New Initiatives and Policies Page Now Available
NIH posted an Implementation of New Initiatives and Policies page on the NIH Grants & Funding Website to pull together the latest information on recent and upcoming changes that impact applications and grants administration.
Page Highlights
Bookmark the link, share it widely, and visit regularly for updated information.
Questions? grantsinfo@od.nih.gov
Categories: New Resources
Topics: Grants Policy and Compliance
{kind=link}
{kind=link}
{kind=link}